By Calvin J. Kersbergen and Bryan K. Ward, M.D.
Ménière’s disease is a disorder of the inner ear consisting of intermittent, spontaneous episodes of vertigo (dizziness) in combination with other fluctuating ear symptoms including low-frequency sensorineural hearing loss, aural fullness, and tinnitus. The condition is associated with Prosper Ménière who in 1861 identified the inner ear labyrinth as a likely source for symptoms of a syndrome involving episodic vertigo and hearing loss. The cause of Ménière’s disease remains unclear.
Endolymphatic hydrops is a swelling of the endolymph (fluid) spaces that has been observed consistently in postmortem studies of patients with a history of Ménière’s disease, by examining their tissues and cells (known as histology). But hydrops can also occur in asymptomatic individuals and in association with other diseases, suggesting that while hydrops is associated with Ménière’s disease, it may not cause the disorder.
Since it was first discovered, Ménière’s disease has been a disorder managed primarily by otolaryngologists, also known as ear, nose, and throat specialists, or ENTs. As a result, surgical treatments have accompanied attempts at medical management. Inspired by patients' sensations of ear fullness and later by the histologic findings of hydrops, surgeons began manipulating the membranous labyrinth to relieve episodes of vertigo while attempting to preserve hearing. The membranous labyrinth lies within the bony labyrinth and is filled with endolymph fluid.
Published in Frontiers in Neurology in December 2021, our review highlights this history of manipulation of the membranous labyrinth. (See illustration below.) The studies involving patients are uniformly retrospective, with some procedures performed first in animal models of endolymphatic hydrops.
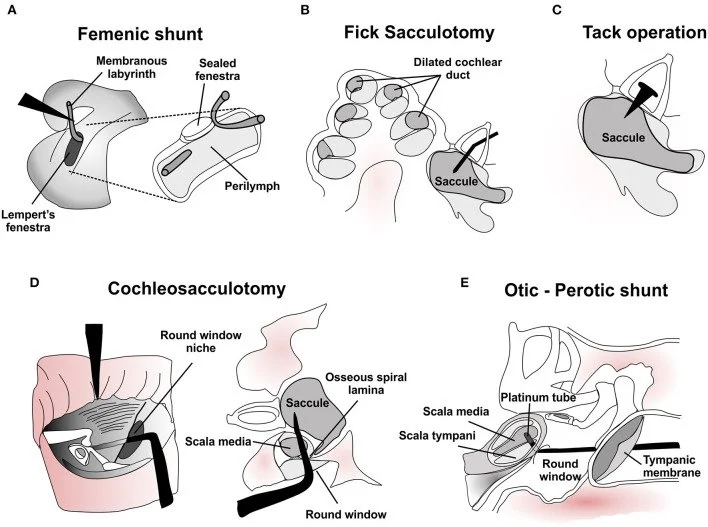
Surgical manipulations of the membranous labyrinth for treatment of Ménière’s disease. (A) Depiction of Femenic's shunt in the lateral semicircular canal to relieve endolymphatic hydrops and vertigo episodes. Adapted with permission from Femenic. (B) Histological representation of endolymphatic hydrops in the cochlear duct and saccule, with a Fick sacculotomy needle placed through a fenestration in the stapes to drain excess endolymph. (C) Permanent tack placement in the stapes bone was intended to enable repeated decompression of the hydropic saccule in the Cody tack operation. (D) Two views of the cochleosacculotomy procedure, where a 90-degree pick is driven through the round window to rupture the cochlear duct and saccule and create a permanent fistula in the osseous spiral lamina. Adapted with permission from Schuknecht and Kinney et al. (E) Depiction of the Otic-Perotic shunt procedure, where a platinum tube is placed in the basilar membrane of the basal cochlea to enable decompression of the scala media. Adapted with permission from Pulec. Photo credit: Copyright © 2021 Kersbergen and Ward, Frontiers in Neurology. Please refer to the paper for additional references.
These procedures indicate a rich history of innovation that parallels developments in otologic surgery. Lateral semicircular canal fenestration, the introduction of the operating microscope, the development of stapes surgery, and now increasing experience with semicircular canal plugging have each influenced procedures that aim to address the finding of endolymphatic hydrops. Some use a minimally invasive technique, in many cases performed using only local anesthetic.
The broad goals of these procedures are eliminating episodic vertigo while preserving hearing. Assessing the success of interventions is difficult due to the natural history of Ménière’s disease in which cessation of vertigo episodes over time is common. Also, whether the procedures improved endolymphatic hydrops specifically was unknown, since historically this could be assessed only by histology on postmortem specimens.
While hearing loss remains frequent following these procedures, many individuals who underwent procedures experienced relief from vertigo without hearing loss. Again, this relief might have occurred despite the intervention, but other variables such as technical differences among surgeons and other patient-specific factors like the extent of hydrops may underlie undesirable complications and variable outcomes.

Advances in surgical technology—such as preoperative imaging, operative robotics, and improved magnification—will lead to new surgical approaches on the membranous labyrinth. Our hope is that this also will improve outcomes for patients with inner ear disorders like Ménière’s disease.

Calvin J. Kersbergen (above left) is an M.D./Ph.D. candidate at Johns Hopkins University School of Medicine, where 2020 Emerging Research Grants scientist Bryan K. Ward, M.D. (bottom left), is an assistant professor of otolaryngology–head and neck surgery.
The Latest Blog Posts




Although it’s one of our most important connections to the world around us, most people don’t routinely monitor changes in their hearing, track exposure to excessive noise, or include hearing screenings as part of their regular preventative care.